
When the bowl finishes before the meal does — what’s actually happening when your frenchie or pug eats fast
Your frenchie inhales his food in forty seconds. The pug doesn’t pause to breathe between bites. Hours later, between meals, there’s the diarrhoea, the bringing-up, the noise the airway makes that the daytime didn’t have. You’ve been told a version of the cycle: small dogs eat too fast, the food empties too fast, nothing absorbs, the dog’s hungry again, eats fast again.
If you’ve watched the cycle, you’re not imagining it — and the answer the wellness category gave you isn’t quite the answer the canine research carries. How fast he eats isn’t the mechanism the category claims. The mechanism that holds up is upstream of that — what comes back up after the bowl, not what fails to absorb on the way down.
What the upper-aerodigestive research backs up as the brachycephalic mechanism is what’s here — and what that means for what you actually do at home. The difference matters because slow feeders, smaller meals, and raised bowls sit in a different relationship to the mechanism that holds up than they do to the category’s story.
Why does my frenchie or pug eat so fast?
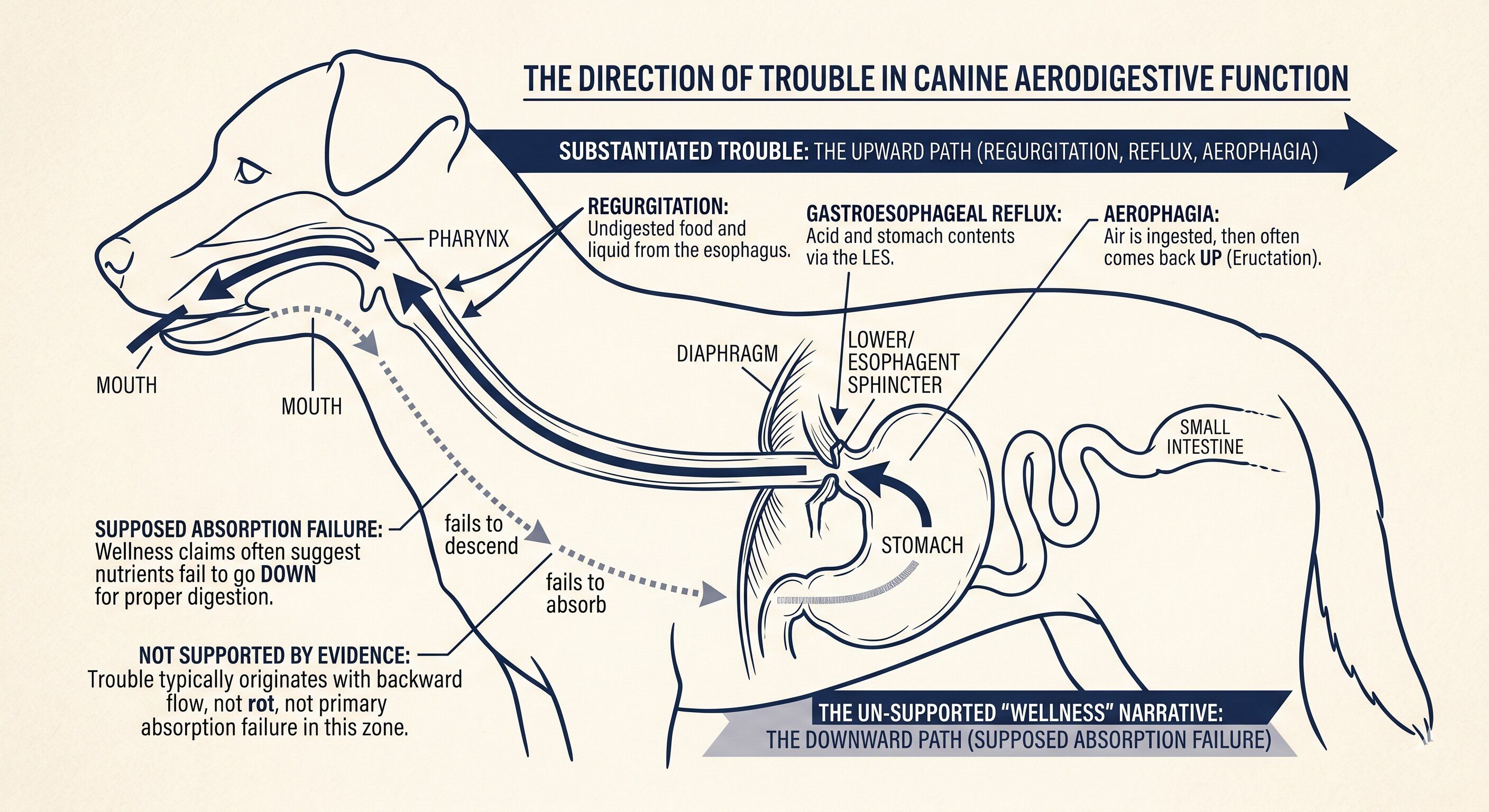
Fast eating is one consequence of the anatomy — so is a food pipe that doesn't push things down properly, stomach acid that comes back up, and air swallowed with every meal. The fast eating is real. What the research doesn't support is the explanation most brands attach to it: that eating quickly means the stomach empties too fast, which means nutrients don't get absorbed. The wellness category's explanation — that small dogs eat too fast, empty too fast, and can't absorb — isn't what the canine research backs up.
Why does my brachycephalic dog vomit between meals?
What you're seeing is most often regurgitation — food coming back up passively, not active vomiting that happens before proper digestion even starts. Two large studies found that virtually all French Bulldogs have some form of this going on: their facial structure doesn't just affect the airway, it puts strain on the food pipe and stomach, too. Reflux, aerophagia (swallowed air), and sliding hiatal hernia (the stomach intermittently moving up through the diaphragm) are all documented in brachycephalic dogs, and any of them can produce what you're seeing. The food didn't fail to absorb. It didn't always stay down long enough to try.
Do slow feeders actually help brachycephalic dogs?
Slow feeders are sensible. They aren’t proven. The brachycephalic-specific intervention research hasn’t shown they work. Owners who use slow feeders, smaller meals, and raised bowls are doing sensible, practical management that may help — and that’s worth respecting at face value. What it isn’t is a proven mechanism. The discipline is to honour what parents are already doing without overclaiming what’s been shown.
Are pugs and frenchies the same when it comes to food handling?
No — at the airway-geometry level they're meaningfully different. In the same study, 16% of Pugs showed digestive symptoms — compared to 93% of Frenchies. Pugs have less room in the upper airway; Frenchies' tongues sit differently against the throat. The research describes the difference. It hasn't explained why.
What does “eats too fast” actually do?
The wellness narrative runs like this: a small dog inhales food because the meal is small and the dog is built fast. The food empties through the small stomach too quickly. There isn’t enough time to absorb. The dog stays hungry. The cycle repeats.
The canine literature — the gastric-emptying studies that have actually measured this — runs the other way. The study found gastric emptying is inversely related to body weight: smaller dogs empty slower, not faster. A 2010 study using a tracking device that the dog swallows found the same pattern. So the "eats too fast, empties too fast, can't absorb" explanation that the category leans on doesn't match what the research measured.
This isn’t a critique of the owners or the vets who repeat the cycle. The cycle is a story that makes intuitive sense — fast in, fast out, nothing in between. The literature just shows it isn’t the right story. The cycle exists in the dog. The explanation for it has been pointing in the wrong direction.
What does brachycephalic conformation actually do at the bowl?
Brachycephaly is a structural condition the airway carries — the shortened skull, the soft palate that sits where it shouldn’t, the laryngeal anatomy working with less room. What the canine research has been measuring more recently is that the same structural condition reaches into the upper aerodigestive layer.
What that produces is a set of mechanisms that hold up. Esophageal dysmotility — the swallowing muscles don’t always coordinate cleanly¹. Gastroesophageal reflux — measured directly in brachycephalic dogs by pH probe². Aerophagia — swallowed air, much more common in brachycephalic dogs than in non-brachycephalic ones³. Sliding hiatal hernia — the upper stomach moving above the diaphragm on and off⁴. And, in the surgical research, regurgitation between meals as a documented sign — 93% of French Bulldogs in the Kaye 2018 study showed at least one gastrointestinal sign⁵; 100% of French Bulldogs in the Bottero 2025 endoscopy series had at least one gastrointestinal endoscopic finding⁶.
What you've watched — the vomiting between meals, the loose stools — maps onto this. The vomiting between meals is usually food sliding back up before it had a chance to digest. It didn't fail to absorb. It didn't stay down long enough to start. The loose stools sit alongside it — a real observation, worth watching, and worth reading more about. But the evidence doesn't point to it being a flat-faced-breed problem specifically. That's a distinction worth keeping.
The breath reports what the gut couldn’t finish.
What does the dog tell you and what does the body actually carry?
One finding from the same research is worth sitting with. The study measured actual acid reflux in flat-faced dogs using a pH probe — not reported symptoms, but what was physically happening inside. Then it asked: what can you observe from the outside that would tell you how bad the reflux is? The owner's read on the digestive symptoms couldn't predict it. The severity of the breathing problems couldn't. The degree of throat collapse couldn't. Whether the dog had already had airway surgery couldn't.².
The dog snoring louder isn't necessarily the dog whose reflux is worse. What you can see doesn't map cleanly onto what the body is carrying. Reflux doesn't always look like reflux. The brachycephalic burden runs internally — and what shows at home doesn't always match how heavily the body is carrying it. No obvious distress isn't an all-clear. Obvious distress isn't a clean measure of how bad it is. The body is the better reporter. Even then, what it shows you is only part of what's happening.
What this means in practice is that the reading runs in both directions. The dog who looks fine may be carrying more than you can see. The dog who looks like she’s struggling may be carrying less than the noise suggests. What you need isn’t a louder read; it’s a longer one.
This is also where the brachy-margin reminder lands. Brachycephaly works as a structural disease state, not a different physiology — what differs is the conformation, and what the conformation produces is constraint turned up louder. At the cooling system. At the airway. In flat-faced breeds, the margin is tighter still — backed up, now, across all three.
What can you actually do?
This is where the discipline gets careful, because what comes next is what the wellness category broadly says — slow feeders, smaller meals, raised bowls, switching up the food form — and the research on those, in brachycephalic dogs specifically, is thin.
The honest framing is practical management. Slow feeders haven’t been measured against pH-probe outcomes or VFSS swallowing studies in brachycephalic-specific intervention trials. Same caveat for raised bowls, smaller meals more often, kibble-shape changes. None of these are mechanism-proven brachy interventions; all of them are reasonable things to try that may or may not move the needle for the dog in front of you. Try them; watch; keep what helps; let go of what doesn’t.

The breed difference matters here too. French Bulldogs and Pugs aren’t the same dog with the same face. Frenchies, in the surgical research, carry the gastrointestinal burden most heavily — 93% of Frenchies in Kaye 2018 had gastrointestinal signs. Pugs in the same study had 16%⁵. The Pug airway has its own geometry — smaller nasopharyngeal cross-sectional area⁷, smaller normalised tongue volume⁸, and the main pattern is airway-restriction-led rather than upper-gastrointestinal-led. The 16% versus 93% difference is described in the research; no published work has yet mapped airway geometry onto symptom prevalence, so the difference holds as a description rather than an explained mechanism. If your dog is picky in a way that looks behavioural but might be reflux, the F→C reflux-as-pickiness pipeline is the next read.
If the regurgitation is severe, frequent, or comes with laboured breathing, weight loss, or aspiration risk, the diagnostic and management territory belongs in vet hands — pH probe, endoscopy, sliding-hiatal-hernia evaluation, sometimes a surgical pathway. The reframe here holds for what you read at home; the calibration holds for the dog whose burden you can see.
Where TENDS sits in this question
Superfood Blend is density-tuned and made for small bodies — the same food principle holds across breeds; brachycephalic conformation makes the bowl-finishes-before-the-meal-does pattern more visible, not the food itself different. Hydration Ritual GUT supports digestive harmony from within, on the whole-body side of what the upper-gastrointestinal burden carries. Neither is positioned as a brachycephalic intervention — there is no mechanism-proven brachy-specific food and TENDS doesn’t claim one. They sit alongside as the kind of food and hydration that holds the small-body system, with the brachy parent able to read the system and choose. Where the reflux is bad enough that the food alone can’t reach it, the vet-prescribed pathway is where to be.
What stays down, and what doesn’t
The diarrhoea between meals, the noise after the bowl, the bringing-up that comes hours later, the bile in the morning — they map onto two different things. Some of it is what he eats. More of it, with these breeds, is what comes back up.
What goes down doesn’t always stay down. What the bowl finishes, the airway sometimes can’t.
Read the dog. Not the chart.
Sources
1. Eivers C, Chicon Rueda R, Liuti T, Salavati Schmitz S (2019). Retrospective analysis of esophageal imaging features in brachycephalic versus non-brachycephalic dogs based on videofluoroscopic swallowing studies. Journal of Veterinary Internal Medicine, 33(4), 1740–1746. https://doi.org/10.1111/jvim.15547 2. Appelgrein C, Hosgood G, Thompson M, Coiacetto F (2022). Quantification of gastroesophageal regurgitation in brachycephalic dogs. Journal of Veterinary Internal Medicine, 36(3), 927–934. https://doi.org/10.1111/jvim.16400 3. Grobman M, Krueger D, Lever TE, Reinero CR (2024). Incidence and characterization of aerophagia in dogs using videofluoroscopic swallow studies. Journal of Veterinary Internal Medicine, 38(3), 1632–1641. https://doi.org/10.1111/jvim.17054 4. Luciani E, Reinero C, Grobman M (2022). Evaluation of aerodigestive disease and diagnosis of sliding hiatal hernia in brachycephalic and nonbrachycephalic dogs. Journal of Veterinary Internal Medicine, 36(4), 1229–1236. https://doi.org/10.1111/jvim.16485 5. Kaye BM, Rutherford L, Perridge DJ, Ter Haar G (2018). Relationship between brachycephalic airway syndrome and gastrointestinal signs in three breeds of dog. Journal of Small Animal Practice, 59(11), 670–673. https://doi.org/10.1111/jsap.12914 6. Bottero E, Ferriani R, Bottero D, et al. (2025). Clinical evaluation and systematic classification of endoscopic gastrointestinal findings in 176 French Bulldogs with brachycephalic airway obstructive syndrome. Animals, 15(14), 2137. https://doi.org/10.3390/ani15142137 7. Heidenreich D, Gradner G, Kneissl S, Dupré G (2016). Nasopharyngeal dimensions from computed tomography of Pugs and French Bulldogs with brachycephalic airway syndrome. Veterinary Surgery, 45(1), 83–90. https://doi.org/10.1111/vsu.12418 8. Siedenburg JS, Dupré G (2021). Tongue and upper airway dimensions: a comparative study between three popular brachycephalic breeds. Animals, 11(3), 662. https://doi.org/10.3390/ani11030662
Written by the TENDS Nutrition & Research Team
Built within the TENDS small-breed formulation and behavioural framework
Big Brand? No.
A Smaller One — On Purpose.
Stay close for bold new moves in small-breed care.
RESET
